
Article 2 – Health Care Program Governance
1.2.3 Quality Management Program Overview
-
Background
-
California Correctional Health Care Services (CCHCS) delivers a continuum of health care services to patients by different professional disciplines across multiple levels of care in both outpatient and inpatient settings. In order to improve care and avoid unnecessary morbidity, mortality and costs, health care and correctional staff need to implement sustainable strategies that:
-
Improve processes and systems to ensure high reliability and sustainability.
-
Strengthen continuity and coordination of care.
-
Strengthen communication and collaboration among all professional disciplines and with the patient.
-
-
An overarching strategy that CCHCS has endorsed to improve patient care and system performance is the establishment of a primary care management model, which is a collaborative care model that is different than the traditional medical model that organizes services around acute and episodic events. Rather, the primary care model provides continuous services to patients with chronic and complex physical and behavioral health conditions who disproportionately drive risk and resources.
-
The Primary Care Model is based on a number of nationally recognized models and paradigms that emphasize:
-
Risk stratification of individual patients and patient populations using a classification system that determines each patient’s health care risk and places the patient at a facility best equipped to manage his or her health care needs in a cost effective manner.
-
A Comprehensive patient focus.
-
Interdisciplinary and consistent team-based care.
-
Evidence-based practices.
-
Active patient involvement and self-management.
-
Decision support and information systems to assist in managing individual patients and patient populations, and facilitating continuous improvements in patient outcomes, clinical practice and processes of care.
-
-
-
Policy
-
Consistent with private and public health care industry standards, CCHCS maintains a Quality Management (QM) Program to continuously evaluate and improve the performance of the health care system. The design of the QM Program draws from nationally recognized quality improvement organizations, principles, concepts, and models.
-
To support health care staff in consistently delivering timely, effective, efficient, and safe care, the QM Program:
-
Supports the identification of performance improvement priorities, and requires development of performance improvement plans and objectives at statewide and institution levels.
-
Provides structures, processes, tools and techniques to analyze and redesign health care processes and manage change.
-
Assists institutions in establishing, improving, and sustaining an integrated health care delivery system.
-
Maintains a performance evaluation program, including an organization Health Care Services Dashboard (Dashboard), and ongoing business intelligence to assess critical health care processes and outcomes, identifying potential areas for improvement, and evaluating performance at all levels of the organization.
-
Requires and provides Patient Registries, evidence-based guidelines, training, and deployment of improvement models and tools such as Focus-Plan-Do-Study-Act (Focus-PDSA) as elements of the performance improvement program.
-
Promotes a culture of teamwork and continuous learning and innovation.
-
-
The scope of the QM Program includes clinical operations, clinical practice, and program administration across all health care delivery settings. The specific priorities of the QM Program change but always strategically focus on key performance areas that most impact the access, quality, safety, utilization, cost, and value concerns.
-
-
Purpose
-
To support continuous health care system evaluation and positive change in order to:
-
Improve patient outcomes.
-
Improve health care quality, cost effectiveness, and patient and staff safety.
-
Improve cost-efficiencies and value-added work, and reduce waste.
-
Comply with legal and regulatory requirements.
-
-
Responsibility
-
Chief Executive Officers (CEOs) oversee implementation of the QM Program at the local level, and participate in statewide strategic planning and implementation and evaluation of statewide initiatives. Institutions may have a local Chief Quality Officer who provides subject matter expertise and supports implementation of the QM Program locally.
-
The Receiver, CCHCS, and Director, Division of Correctional Health Care Services delegate responsibility for statewide planning, implementation, and evaluation of the QM Program to the statewide Chief Quality Officer.
-
-
Quality Management Program
-
Identifying Improvement Priorities and Strategic Alignment
-
Overview
-
Improvement efforts are most effective when all levels of an organization are informed of improvement priorities and rally around a core set of improvement goals. To this end, the QM Program facilitates the setting of improvement priorities at the statewide level and provides support to institutions as they identify institution-specific priorities, communicate priorities to health care staff, and ensure that program planning and day-to-day operations align with improvement priorities.
-
-
Priority-Setting Process
-
Each year, CCHCS reviews health care areas considered to be high risk, high volume, high cost, and problem-prone and identifies organization-wide improvement priorities. CCHCS incorporates the highest-priority program areas or topics into a performance improvement plan, with one or more performance objectives established for all priority improvement areas. The development and pre-implementation vetting process involves health care leadership as well as external stakeholders. This same priority-setting process occurs at each institution:
-
Taking into consideration statewide strategic priorities and the Primary Care Model, institutions identify institution-specific improvement priorities and performance objectives, customizing an institution improvement plan for the facility’s health care mission, resources, and the needs of the patient population which is vetted through statewide leadership via the Quality Management Committee (QMC) and other forums.
-
The QM Program promotes the establishment of clear and measurable performance objectives for all improvement initiatives and sustainability planning to ensure that successful improvement strategies and positive results can be reproduced consistently in the future.
-
Upon developing an annual improvement plan, institution leadership is responsible for communicating improvement priorities to staff at all levels of the health care system and helping staff understand their role in achieving improvement objectives.
-
Institution leadership also guides the process of strategic alignment, by which managers and supervisors determine how program operations and day-to-day supervision will support performance objectives, and how care teams and other staff incorporate improvement activities for priority areas into day-to-day work.
-
-
-
Performance Evaluation
-
Overview
-
To assess the impact of change management efforts and progress toward performance objectives, CCHCS uses an objective and systematic process to measure and evaluate health care system performance. Taking into consideration the organizational mission and patient population risks and needs, CCHCS determines the clinical and administrative processes that are most important to measure, and chooses structural, process, and outcome measures critical for ongoing monitoring of the health care system and identification of quality improvement opportunities.
-
In determining performance measures, CCHCS considers the science or evidence supporting the selected measures, and comparable measures used broadly in the health care industry, including those employed by the Healthcare Effectiveness and Information Set and the Agency for Healthcare Research and Quality. Among other factors, the CCHCS takes into account the performance of other health care organizations and past organizational performance during the establishment of performance objectives.
-
-
Performance Evaluation
-
CCHCS consolidates key performance measures essential to fulfilling the organization’s mission in the Dashboard, a monthly organization-wide report widely distributed to health care staff. All performance improvement plan objectives are benchmarked and monitored through the Dashboard. The Dashboard provides performance data at statewide and institution levels, and trends performance over time.
-
In addition to the monthly Dashboard, CCHCS uses other methods to evaluate performance and inform decisions about improvement priorities, including, but not limited to:
-
Periodic performance reports and special studies, including morbidity and mortality analysis.
-
A health incident reporting system and a defined process for the tracking, analysis, and reporting of sentinel events.
-
Standardized audit tools to evaluate the quality of care and assess adherence to practice guidelines, policies and procedures, and federal and state laws.
-
Patient Registries or “exception reports” that identify individual patients who have not received services per treatment guidelines or who have abnormal findings.
-
-
CCHCS ensures that there are appropriate processes in place to validate performance data, particularly when:
-
A new measure is introduced or an existing measure is substantially changed.
-
Data will be made public on the internet or through other mechanisms.
-
There are unexpected changes in the data reported for an existing measure.
-
Data sources change (e.g., paper-based records become electronic).
-
-
-
Performance Data Validation
-
Validation processes may include, but are not limited to, use of statistically-valid samples, redundant data collection by independent parties, and corrective actions to address data discrepancies.
-
-
-
Performance Improvement Models, Tools, and Training
-
Overview
-
Consistent with health care industry standards, the QM Program uses the science of process improvement and change management, including techniques and tools, to assist health care staff in establishing and maintaining an integrated health care delivery system and achieving objectives outlined in improvement plans. The CCHCS QM Program promotes:
-
Establishing clear and measurable objectives for all improvement initiatives.
-
Using decision support such as care guides, chart review tools, forms, and checklists, and staff development programs, such as continuing education presentations, workshops, and on-the-job training to remind care teams of evidence-based guidelines and reinforce new health care processes.
-
Using information systems, such as the Dashboard, Institution Scorecard, Patient Registries, provider profiles, performance reports, and tracking systems to support proactive administrative and clinical management.
-
Re-evaluating critical health care processes on a regular and ad hoc basis through mechanisms such as Root Cause Analysis and Failure Mode and Effects Analysis, and redesigning processes and systems to improve outcomes.
-
Engaging patients as active and responsible participants in the health care process through patient education and self-management programs, and partnership with peer educators and incarcerated person groups such as Men’s/Women’s Advisory Council.
-
Formally documenting new processes, such as in a local operating procedure, ongoing use of decision support, orientation for new staff, and regular training updates for continuing staff to promote lasting and sustainable change.
-
-
Improvement Models
-
CCHCS uses the Cycle of Change Model as a framework for design and implementation of improvement initiatives at both the state and institution levels. The Cycle of Change Model is based on a number of Performance/QM models and the Chronic Care Model that support behavioral change and sustainable business processes that promote the Primary Care Model. Under the Cycle of Change, institutions:
-
Identify improvement priorities,
-
Set performance objectives,
-
Clarify performance expectations and create decision support to help staff meet performance expectations,
-
Provide training and staff development,
-
Provide targeted technical assistance from managers, supervisors, designated mentors or “champions” or other staff in areas where performance continues to lag, and
-
Regularly re-assess performance to determine progress toward performance objectives.
-
-
Within the health care and quality improvement industries, there are other established methods which include statistical analysis, Root Cause Analysis, the Model for Improvement, Lean Model, Six Sigma, Focus-PDSA, Failure Mode and Effects Analysis, Process Flow Diagramming, and Cause and Effect Diagramming for analysis of performance problems, development of solutions, and testing and evaluating interventions.
-
These improvement models provide a framework for redesigning health care processes and implementing improvement initiatives at the point of care, such as incorporating decision support and information systems into day-to-day practice.
-
-
Training on Quality Improvement Techniques
-
CCHCS, through the QM Program, is responsible for educating health care staff about improvement models, helping staff to develop the skills to use these models, and developing toolkits that support health care staff step-by-step through the application of an improvement model or concept.
-
-
-
Technical Assistance from Headquarters and Regional Staff
-
CCHCS staff based at headquarters and at regional levels support institutions as they redesign health care processes and establish well-functioning QM Programs.
-
Among other activities, headquarters-based staff and regional teams from various disciplines and program areas:
-
Assist institutions in identifying improvement priorities and developing improvement plans.
-
Review program performance data, evaluate the effectiveness of quality improvement interventions, assess the performance of the integrated health care services delivery system, and determine progress toward performance objectives.
-
Perform quality of care reviews and assist institutions in planning and implementing activities to improve the quality of clinical practice.
-
Support the institution in taking action when quality or safety problems are identified including, but not limited to, sharing best practices and participating in improvement teams.
-
Assist institutions in preparations for licensing surveys, audits by external stakeholders, and inspections, and as they develop and manage implementation of improvement plans.
-
Promote adherence to policies, evidence-based guidelines, and standards of care through development of decision support tools and staff development programs, among other strategies.
-
Ensure dissemination of relevant, accurate, and timely performance information to institution management and staff.
-
Review QM governance activities and recommend program changes or further activity.
-
Identify, disseminate, and adapt best practices.
-
Support local staff development programs to orient all health care staff to the QM Program, promote the skills necessary to perform quality improvement work at institutions, and empower staff at all reporting levels to participate in quality improvement.
-
-
-
-
Quality Management Program Governance
-
Overview
-
The QM Program includes a management structure composed of inter-disciplinary committees and teams at statewide and local levels to support organizational communication, coordination, control and change. The organization’s leadership uses the QM Program management structure to:
-
Plan, implement, evaluate and improve the health care system’s performance.
-
Oversee quality improvement and patient safety initiatives.
-
Coordinate improvement activities across programs and disciplines.
-
Communicate strategic direction and measurement information.
-
Ensure orientation and training of staff as it relates to performance and quality improvement.
-
Promote a culture of continuous learning and innovation.
-
-
The committee network serves as a supplement to the traditional reporting structure at headquarters and at individual institutions, providing regular interdisciplinary forums for managers, supervisors, and line staff to manage improvement activities.
-
-
Quality Management Committees
-
The statewide QMC meets at least quarterly and the institution QMC meets at least monthly to determine improvement priorities and strategies, regularly review performance data and take action to improve performance, coordinate the activities of committees and teams that focus on process and performance improvement, and ensure that staff are trained in quality improvement concepts, tools, and techniques.
-
Quality Management Committees ensure that staff at the headquarters and local level receives the orientation and training necessary to participate in improvement activities and apply improvement skills, such as problem analysis and system redesign, in their day-to-day work.
-
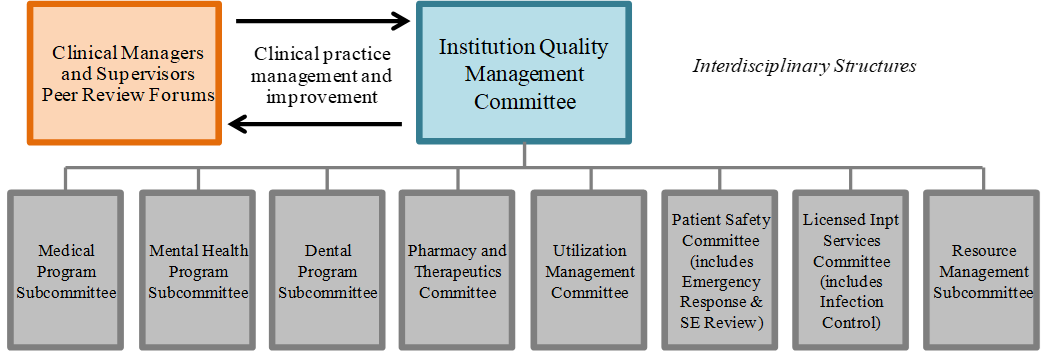
At the institution level, a defined network of program subcommittees, many of which are required by departmental policy or health care licensing regulations, perform the same types of activities as the institution QMC, but within a discreet program area, with reporting requirements to the institution QMC. Appendix 1, Program Specific Subcommittees, provides a matrix of program-specific subcommittees with references to requirements in department policy and state law. Figure 1 shows common subcommittees at the institution level.
-
All standing performance committees and subcommittees have the capacity to form Quality Improvement Teams (QITs), which are time-limited, multi-disciplinary teams convened to analyze and address a particular program or process performance problem. QITs will provide regular updates to the committee that chartered them including a final report at the close of the improvement initiative.
-
All local QMCs report to and receive direction from the statewide QMC. At some institutions, the QMC also reports to a Local Governing Body to meet regulatory requirements, which can serve as an opportunity to promote strategic management of the health care system and prison by the CEO, Warden, and their leadership.
-
Figure 1: Institution Quality Management Program Governance
-
-
-
-
Appendices
-
Appendix 1: Program Specific Subcommittees
-
-
References
-
The design of the QM Program draws from nationally-recognized quality improvement and patient safety organizations, principles, concepts, and models, including:
-
Joint Commission on Accreditation of Hospitals
-
The Care Model
-
Patient-Centered Medical Home
-
International Organization for Standardization (ISO) 9000:2000 standards
-
Institute of Medicine
-
Institute of Healthcare Improvement (Model for Improvement)
-
Baldrige Award Criteria for Process Management and Results
-
Six Sigma
-
Hospital Corporation of America (Focus-PDSA)
-
James Womack (Lean Thinking)
-
W. Edward Demings (Fourteen Points for Managing Quality)
-
Walter J. Shewhart (Cycle for Continuous Improvement)
-
Avedis Donabedian (Structure-Process-Outcome Paradigm)
-
Joseph M. Juran (Pareto Analysis and Juran Quality Trilogy)
-
American Society of Quality
-
-
-
Revision History
-
Effective: 01/2002
Revised: 12/2012
-
-
Appendix 1
-
Program Specific Subcommittees
-
Institution Governance Structure Detail
Committee Applicable Mandates Meeting Frequency Reporting Quality Management Committee HCDOM Section 1.2.3, Quality Management Program (Plata Order)
HCDOM Section 1.2.4, Quality Management Program, Statewide Governance (Plata Order)
HCDOM Section 1.2.5, Quality Management Program, Institution (Plata Order)
NCCHC Multidisciplinary QIC: NCCHC Standards, P-A-06; NCCHC Standards Appendix B; NCCHC Standards Appendix G.
NCCHC Administrative Meeting: NCCHC Standards, P-A-04.Monthly Health Care Services Quality Management Committee, also the Local Governing Body at some institutions with licensed beds Medical Program Subcommittee Quality Management Committee Mental Health Program Subcommittee Mental Health Services Delivery System Program Guide, Chapter10. Suicide Prevention and Response. (Coleman Order) Monthly Quality Management Committee Dental Program Subcommittee HCDOM Section 3.3.4.4, Dental Program Subcommittee (Perez Order) Monthly, or more frequently as necessary Quality Management Committee Pharmacy and Therapeutics Committee Title 22, Division 5, Chapter 12, Article 5, Section 79781 Required Committees.
HCDOM Section 1.2.11, Systemwide Pharmacy and Therapeutics Committee (Plata Order)Not Identified Quality Management Committee Utilization Management Specialty Services Committee Title 15, Division 3, Chapter 2, Subchapter 2, Article 1, Section 3999.200 Provisions of Care and Treatment Exclusions.
Title 15, Division 3, Chapter 1, Subchapter 4, Article 8, Section 3352 Institutional Utilization Management Committee
Title 15, Division 3, Chapter 1, Subchapter 4, Article 8, Section 3352.1 Headquarters Utilization Management Committee
HCDOM, Section 1.2.15, Utilization Management Program (Plata Order)Monthly Quality Management Committee Patient Safety Committee (includes Emergency Response and Sentinel Event Review) HCDOM, Chapter 3, Article 7, Emergency Medical Response (Plata Order) At least monthly Quality Management Committee Licensed Inpatient Services Committee (includes Infection Control) Title 22, Division 5, Chapter 12, Article 5, Section 79781, Required Documentation
HCDOM Sections 1.2.3-1.2.5, Quality Management ProgramAt least annually Quality Management Committee Resources Management
SubcommitteeNot identified Quality Management Committee
-