
Article 2 – Health Care Program Governance
1.2.5 Quality Management Program, Institution
-
Purpose
-
To describe strategies, processes, tools, and a governance structure that institutions use to plan, prioritize, develop, implement, and evaluate performance improvement initiatives and sustain improvements.
-
-
Responsibility
-
The Institution Chief Executive Officer (CEO) is responsible for implementation of this procedure.
-
-
Procedure
-
Performance Improvement Plan
-
Integrated Health Care Services Delivery System
-
Implementation of an integrated health care services delivery system with a strong primary care foundation has been identified as an overarching strategy for improving care and avoiding unnecessary morbidity, mortality, and costs. Health care staff at each institution are responsible for implementing care processes necessary for a sustainable integrated health care delivery system including, but not limited to, processes to:
-
Identify the health risk of each patient and ensure that the patient is placed at an institution and/or treatment setting with the capacity to address his or her health care needs, per an automated Clinical Risk Classification process.
-
Establish consistent interdisciplinary care teams that assume primary responsibility for the patients assigned to them.
-
Provide care coordination for patients as they move from one treatment setting to another, including transitions between care teams, and across levels of care.
-
Ensure that care teams work across disciplines to co-manage each patient as appropriate to his or her health needs.
-
Ensure care teams have necessary resources and information, such as updated health records, specialty care reports, discharge summaries, diagnostic study results, and patient registries, to provide planned care for patients.
-
Provide evidence-based care that is consistent with current guidelines and community standards.
-
Enhance access to services through open access appointments or other scheduling strategies, after-hours care, and effective communication techniques.
-
Ensure that patients have timely and consistent access to medications.
-
Use Patient Registries to manage subpopulations with specific health risk factors or chronic disease, including high risk patients and mental health patients that are high utilizers of services.
-
Promote patient self-management to improve outcomes.
-
-
Priority-Setting Process
-
Each year, institutions shall review health care areas considered to be high risk, high volume, high cost, and problem-prone, and identify improvement priorities taking into consideration statewide strategic priorities and customizing the plan for the facility’s health care mission, resources, and the needs of the patient population. The annual performance improvement plan shall include the following elements:
-
Priority areas for improvement to be targeted by institution staff in the coming year.
-
Performance objectives for each priority area (generally six to twelve) and associated timeframes.
-
Improvement strategies that will be used to achieve performance objectives.
-
-
Development of an Annual Performance Improvement Plan
-
As a first step in developing an improvement plan, each California Department of Corrections and Rehabilitation institution shall evaluate the health care delivery system and identify gaps in areas such as those listed above.
-
Each institution shall prioritize areas to be targeted in improvement initiatives, set measurable performance objectives for each area, and determine which strategies the institution will use to achieve objectives.
-
Upon developing an improvement plan for the year, institution leadership shall take steps to inform institution staff about the improvement priorities for the year and help managers, supervisors, and line staff to identify specific ways they might contribute to improvement efforts as part of their current duties. To this end, institution leadership is responsible for:
-
Communicating improvement priorities to staff at all levels of the health care system.
-
Helping staff understand their role in achieving improvement objectives.
-
Guiding the process of strategic alignment by which managers and supervisors determine how program operations and day-to-day supervision will support performance objectives and how care teams and other staff incorporate improvement activities for priority areas into their day-to-day work.
-
Updating health care staff about any changes to the improvement plan that occur throughout the year.
-
Keeping institution staff apprised of progress toward meeting objectives in the annual improvement plan.
-
-
-
-
Performance Evaluation
-
Overview
-
As part of the development of an annual improvement plan, each institution shall determine performance measures and objectives for each priority area identified in the improvement plan. Progress toward the achievement of improvement objectives should be monitored at least monthly and regularly conveyed to all health care staff. To make data as useful as possible as a catalyst for change, institutions may consider generating reports that break down performance by:
-
Clinic or care team.
-
Primary Care Provider, Primary Mental Health Clinician, Psychiatrist, or Dentist.
-
Patient subpopulation (e.g., high risk or mental health high utilizers) or other meaningful subgroup.
-
This may help health care staff determine which locations, staff, or patients might receive improvement interventions first, and is generally useful in identifying care teams or individual providers who might present best practices.
-
-
Health Care Services Dashboard
-
For the purposes of identifying opportunities for improvement and potential patient safety concerns, institutions are also required, through Quality Management Committee (QMC) meetings, Quality Improvement Team (QIT) meetings, and other forums, to monitor the performance of critical clinical and administrative processes monthly through the Health Care Services Dashboard (Dashboard).
-
The Dashboard includes institution-level performance data, trended over time, in the form of Institution Scorecards, trended composites, and other data displays. Some of the Dashboard data is derived from institution reports.
-
To ensure that Dashboard data is as useful as possible in informing management decisions, institutions shall take action to ensure accuracy in data reporting including:
-
Ensuring that staff applies standardized methods for data collection, in accordance with statewide policies, procedures, and detailed instructions.
-
Ensuring that staff collecting data are appropriately trained.
-
Periodic data validation through redundant data collection by an independent reviewer (e.g. for clinical practice reviews) and/or checking database information against another data source, such as patient charts to double-check accuracy of health care scheduling data.
-
Conducting inter-rater reliability analysis for reviewers of qualitative data.
-
Use of statistically-valid samples.
-
-
-
Performance Reports
-
In addition to the monthly Dashboard, California Correctional Health Care Services (CCHCS) issues periodic performance reports and special studies including morbidity and mortality analysis.
-
Institution CEOs are responsible for ensuring that these reports are broadly distributed to health care staff and discussed in various meeting forums such as staff meetings and quality improvement committee meetings.
-
-
Patient Registries
-
CCHCS provides lists of patients with targeted dental, mental health, and/or medical conditions to institution staff, updated at least monthly.
-
Patient Registries often include an alert function where patients with abnormal findings or who are missing services required by CCHCS guidelines are highlighted. Institution care teams are required to review registries at least monthly (and more often as appropriate) and take action to follow-up with patients as necessary to improve patient outcomes.
-
-
Data Integrity
-
When an institution determines that there may be a problem with data accuracy, the institution shall immediately notify the QM Section and shall institute corrective actions to ensure data reliability.
-
-
-
Quality Improvement Techniques, Tools and Training
-
Consistent with health care industry standards, institutions shall use improvement processes, techniques, and tools to assist health care staff in establishing and maintaining an integrated health care delivery system, achieving objectives outlined in annual improvement plans, and regularly evaluating and redesigning health care processes. Institutions shall:
-
Establish clear and measurable objectives for all improvement projects.
-
Re-evaluate critical health care processes on a regular basis and redesign operations to implement an integrated health care delivery system and improve outcomes and efficiency.
-
Apply improvement models used widely in the health care and quality improvement industries such as Root Cause Analysis, the Model for Improvement, Lean Model, Six Sigma, Focus-Plan-Do-Study-Act, Failure Mode and Effects Analysis, Process Flow Diagramming, and Cause and Effect Diagramming to analyze performance problems, develop solutions, and test and evaluate interventions.
-
Use Patient Registries to identify and manage high risk patients and patients with specific chronic conditions and standardized decision support tools disseminated by the QM Program such as care guides and quality of care review tools, in the application of improvement processes and techniques.
-
Take steps to sustain improvements when an initiative has proven successful such as memorializing new processes in Local Operating Procedures (LOP) or documenting new staff roles in duty statements.
-
Orient and train staff on QM Program structures, processes, and tools and ensure that staff attends statewide training programs designed to build improvement skills in the field.
-
Take actions to promote a culture of teamwork and continuous learning and innovation.
-
-
The Cycle of Change described in the Quality Management Program Overview presents a framework for the design and implementation of institution improvement initiatives, incorporating the principles described above.
-
-
-
Quality Management Program Governance
-
Overview
-
Each institution shall maintain an interdisciplinary QM Program structure to monitor and direct performance evaluation and improvement activities. The management structure includes standing committees at two levels:
-
An institution QMC that plays a central role in coordinating performance evaluation and improvement activities institution-wide, providing overall strategic direction for the institution quality QM system and communicating performance improvement activities to the statewide QMC.
-
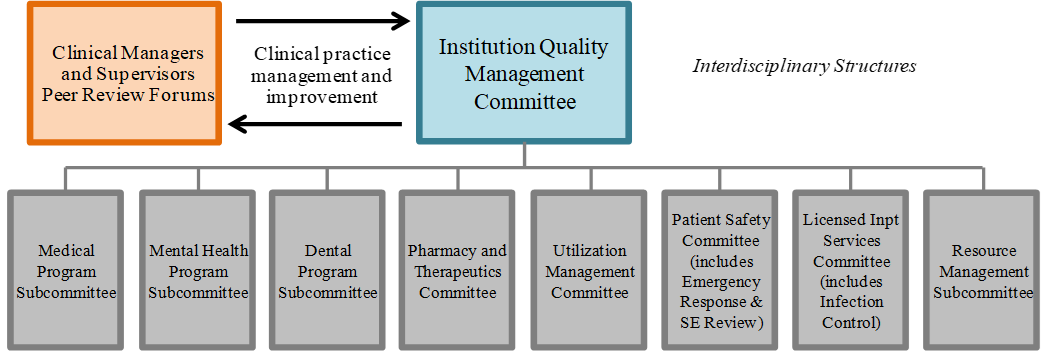
Subcommittees that evaluate performance at the program level, develop program-specific improvement plans and manage implementation of improvement initiatives. Image 1 provides a schematic of the management structure overseen by the institution QMC.
-
-
The institution QMC or any subcommittee may convene a QIT, a multi-disciplinary team charged with addressing a particular improvement opportunity. QITs typically exist for the duration of the improvement project and disband upon completion.
-
Other forums such as staff meetings, weekly provider meetings, Primary Care Team huddles, and monthly all Primary Care Team meetings serve as important conduits of performance improvement information and support implementation of improvement initiatives including, but not limited to:
-
Ensuring all staff understand the elements of the integrated health care services delivery system consistent with the Primary Care Model and the QM system.
-
Communicating annual improvement priorities and objectives.
-
Reviewing performance data, particularly at the clinic or provider level.
-
Disseminating decision support tools and conveying expectations for use.
-
Conducting staff development activities consistent with priority improvement areas.
-
Developing and implementing improvement initiatives, including process redesign, that align with the institution’s improvement priorities and may be specific to a discipline (e.g., health records technicians) or work location (e.g., Yard B).
-
Sharing best practices.
-
Figure 1: Institution Quality Management Program Governance – Standing Committees
-
-
-
Institution Quality Management Committee
-
Overview
-
In general, the institution QMC provides oversight to local performance improvement activities and ensures that health care programs operate in adherence with applicable laws, regulations, policies, procedures, and standards of care; the institution QMC serves as a hub for change management, collaboration, and coordination across programs and disciplines as activities relate to performance management and improvement, and serves as a conduit of improvement and patient safety information from the institution to headquarters.
-
Among other responsibilities, the institution QMC:
-
Evaluates the performance of the integrated health care services delivery system at the institution, including CCHCS Primary Care Model, and directs efforts to improve care.
-
Sets improvement priorities, regularly evaluates program performance and takes action to make improvements, and coordinates the work of multiple standing committees focusing on particular health care programs or functions.
-
Ensures that institution staff is trained in quality improvement concepts, processes, and tools, promotes a culture of continuous learning and improvement at the institution.
-
-
The scope of the institution QMC is separate and distinctly different from the organized medical staff. The role of an organized medical staff at the institution, if it exists, is peer review and addressing individual clinician practice issues in conjunction with management while the institution QMC oversees organization-wide system performance and improvement activities, which requires involvement of all disciplines and line staff, supervisors and managers. (refer to Image 1)
-
-
Committee Actions
-
Specifically, the institution QMC takes on the following actions:
-
Strategic Direction
-
Identifies institution-specific improvement priorities and objectives through the development of an annual performance improvement plan.
-
Aligns institution performance improvement activities with statewide improvement priorities and initiatives.
-
Provides feedback to the statewide QMC on statewide improvement priorities, performance metrics, and initiatives.
-
-
Program Evaluation and Improvement
-
Reviews program performance data, including the organizational Dashboard and Institution Scorecards, statewide performance reports, QIT reports, and reports by outside entities, including the Office of the Inspector General, court monitors, and the Prison Law Office, at least monthly.
-
Uses performance data to identify improvement opportunities, evaluate the effectiveness of quality improvement interventions in the Institution Performance Work Plan, and assess the performance of the integrated health care services delivery system, and determine progress toward performance objectives.
-
Takes action when quality or safety problems are identified incorporating new initiatives in the Institution Performance Work Plan, including assigning interdisciplinary QITs to analyze quality problems, select solutions, and implement quality improvement initiatives.
-
Approves local improvement initiatives for implementation institution-wide and monitor them through the Institution Performance Work Plan including development or modification of health care programs, pilot programs, changes to LOPs, training programs, and development or modification of decision support.
-
Provides oversight during licensing surveys, audits by external stakeholders, and inspections, develops and manages implementation of improvement plans.
-
Oversees implementation of policies, evidence-based guidelines and standards of care.
-
-
Communication and Coordination
-
Ensures dissemination of relevant, accurate, and timely performance information to institution management and staff.
-
Ensures that QMC, subcommittee, and workgroup activities are appropriately documented.
-
Coordinates and reviews subcommittee activities and recommends program changes or further subcommittee activity.
-
Ensures effective communication between local improvement committees, especially in areas of interdisciplinary responsibility or system-wide issues.
-
Identifies and disseminates best practices.
-
Coordinates annual review and approval of institution LOPs.
-
Refer issues to other committees or programs such as the statewide Medical Peer Review Committee when they do not fall under the purview of the QMC.
-
Reports institution performance improvement plans and activities and recommendations for state-level improvements, to the statewide QMC at least annually.
-
-
Orientation and Training
-
Implements and oversees a local staff development program to orient all health care staff to the QM Program, promote the skills necessary to perform quality improvement work at institutions, and empower staff at all reporting levels to participate in quality improvement.
-
-
-
QMC Membership, Meetings, and Reporting
-
QMC Chairperson
-
The institution CEO shall serve as QMC Chairperson.
-
The QMC Chairperson is responsible for ensuring that the QMC meets at least monthly.
-
The committee agenda reflects the responsibilities and actions described in this procedure, program subcommittees report per a designated schedule, and committee decisions are appropriately documented.
-
-
QMC Members
-
The institution QMC shall include the following voting members:
-
Chief Executive Officer
-
Institution CQO
-
Institution Chief Medical Executive
-
Institution Chief Nurse Executive
-
Institution Chief Support Executive
-
Chief, Mental Health Program
-
Health Program Manager III, Dental Program
-
Pharmacist-in-Charge
-
Associate Warden of Health Care
-
Chairpersons of QMC Subcommittees
-
Other members as deemed appropriate such as the Director of Nursing, Supervising Registered Nurse II, Correctional Health Care Services Administrator, Chief Psychiatrist, Supervising Dentist, Nurse Instructor, Public Health Nurse, Health Program Specialists, Standards Compliance Coordinator.
-
-
QMC Meeting Frequency
-
It is recommended that the institution QMC meet weekly. However, at a minimum, the committee shall meet no less than monthly.
-
-
QMC Minutes
-
The Institution QMC shall document each meeting through formal minutes that shall be provided to QMC members for review no later than three business days prior to the next QMC meeting.
-
-
QMC Reporting
-
The Institution QMC reports to and receives direction from the statewide QMC.
-
At some institutions, the QMC also reports to a Local Governing Body to meet regulatory requirements, which can serve as an opportunity to promote strategic management of the health care system and prison by the CEO, Warden and their leadership.
-
-
-
-
QMC Subcommittees
-
Each institution shall maintain subcommittees to establish and sustain high-quality health care services within a defined program area consistent with existing policies and procedures, federal and state law, and community standards of care.
-
A number of standing subcommittees are required by departmental policy or state regulations. Other subcommittees may be established to review and improve performance of a specific program or resource area. Examples of common subcommittees include:
-
Medical Program
-
Mental Health Program, may include Suicide Prevention and Response (also see Patient Safety)
-
Dental Program
-
Pharmacy and Therapeutics
-
Utilization Management
-
Patient Safety
-
Licensed Inpatient Services focuses on compliance with Title 22 of the California Code of Regulations including Infection Control and Patient Care Policy Committees
-
Resource Management including Human Resources, Health Information Management and scheduling systems, Budgets and Physical Space.
-
-
Institutions with licensed facilities may also choose to incorporate the functions of a Patient Policy Committee into the QMC if appropriate.
-
Each Subcommittee Chairperson serves as a member of the QMC and is responsible for reporting subcommittee program performance improvement activities, such as development and implementation of initiatives and improvement projects, to the institution QMC on a routine basis through appropriate documentation (e.g., minutes) and verbal reporting.
-
All subcommittees shall meet as frequently as required in existing policy or state law and meeting minutes shall be completed and readily available for review.
-
-
Quality Improvement Teams (QITs)
-
All standing performance committees and subcommittees have the capacity to form QITs which are time-limited, multi-disciplinary teams convened to analyze and address a particular program or process performance problem.
-
QITs shall provide regular updates to the committee that chartered them and a final report at the close of the improvement initiative.
-
-
-
References
-
California Code of Regulations, Title 22, Division 5, Article 5, Section 79781, Required Committees
-
California Department of Corrections and Rehabilitation, Mental Health Services Delivery System Program Guide, Chapter 10, Suicide Prevention and Response
-
Health Care Department Operations Manual, Chapter 1, Article 2, Section 1.2.11, Systemwide Pharmacy and Therapeutics Committee
-
Health Care Department Operations Manual, Chapter 1, Article 2, Section 1.2.15, Utilization Management Program
-
Health Care Department Operations Manual, Chapter 3, Article 3, Section 3.3.4.4, Dental Program Subcommittee
-
-
Revision History
-
Effective: 01/2002
Revised: 12/2012
-