
Article 1 – Complete Care Model
3.1.6 Population and Care Management Services
-
Procedure Overview
-
The Complete Care Model recognizes that patients have varied health care needs, and the delivery system needs to be flexible enough to serve a wide range of patients – from young, healthy patients without any history of chronic disease, to patients with multiple serious mental health, dental, and medical co-morbidities who require intensive services coordinated across multiple providers. The delivery system shall also include a wide range of social supports to maintain health and functioning.
-
California Correctional Health Care Services (CCHCS) shall provide systematic assessment, risk stratification, monitoring, and care management of identified groups of patients at the statewide, regional, institutional, panel, and individual levels to meet the needs of a diverse patient population. Population management includes the evaluation of resources, processes and outcomes and is an integral component of the Complete Care Model and the Primary Care Team (PCT) function.
-
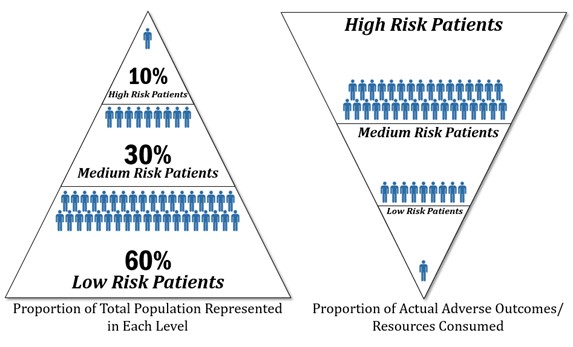
PCTs and other health care staff are expected to provide services to patients commensurate with each patient’s risk level and complexity to protect patients at risk for poor outcomes and ensure the most cost-effective allocation of scarce health care resources. Patients at higher risk utilize the most resources and represent the smallest percentage of the total population. Patients with complex health care needs exposed to the highest risk of permanent disability or death utilize the highest concentration of care management services (refer to figure below).
-
Risk Levels and Actual Adverse Outcomes/Resource Use
-
-
-
CCHCS provides PCTs with guidelines, tools, and reports to support the provision of evidence-based care at all risk levels.
-
This procedure describes the organization’s risk stratification system, specifies the services generally appropriate for patients at different risk levels, and outlines processes for monitoring and managing patient populations, individual patients, and the components of the population and care management services delivery system.
-
-
Responsibility
-
Statewide
-
California Department of Corrections and Rehabilitation (CDCR) and CCHCS departmental leadership at all levels of the organization, within the scope of their authority, shall ensure administrative, custodial, and clinical systems are in place and appropriate tools, training, technical assistance, and levels of resources are available so that Care Teams can successfully implement the Population and Care Management Services Procedure.
-
-
Regional
-
Regional Health Care Executives are responsible for implementation of this procedure at the subset of institutions within an assigned region.
-
-
Institutional
-
The Chief Executive Officer (CEO) has overall responsibility for implementation and ongoing oversight of a system to provide population management which includes risk stratification and care management. The CEO delegates decision-making authority to designated Institutional Health Care Executives for daily operations of the population and care management services system and ensures adequate resources are deployed to support the system.
-
The CEO and all members of the institution leadership team are responsible for ensuring all necessary resources are in place to support the successful implementation of this procedure at all levels including, but not limited to the following:
-
Institution level
-
Patient panel level
-
Patient level
-
-
The CEO and all members of the institution leadership team shall ensure access to and utilization of equipment, supplies, health information system, patient registries and summaries, and evidence-based guidelines.
-
The CEO and all members of the institution leadership team shall ensure protected time at least twice monthly, where each PCT shall conduct a Population Management Working Session utilizing tools such as Dashboards, Master Registries, Patient Summaries to address concerns related to potential gaps in care in order to improve patient outcomes including, but not limited to (refer to the Population Management Working Session Facilitator’s Guide):
-
Trends in access to and quality of care.
-
Patient risk stratification.
-
High risk/complex patients.
-
Patient safety alerts.
-
Resource Management (e.g., contract, supplies, equipment, space, environment).
-
Scheduling Reports.
-
Surveillance of communicable diseases.
-
-
The CEO and all members of the institution leadership team as part of the Quality Management process on an ongoing basis shall:
-
Review and compare institutions’ PCTs performance, including the overall quality of services, health outcomes, assignment of consistent and adequate resources, utilization of Dashboards, Master Registries, Patient Summaries, and decision support tools and address issues as necessary.
-
Provide PCT members with adequate resources, including protected time, staffing, physical plant, information technology, and equipment/supplies to accomplish daily tasks.
-
Work with custody staff to minimize unnecessary patient movement that results in changes to a patient’s panel assignment.
-
-
The Chief Medical Executive (CME) is responsible for overall medical management of patients and ensures resources are available to meet the medical needs of the population.
-
The Chief Nurse Executive (CNE) is responsible for the overall daily clinic operations and ensuring that the institution has designated supervisors to monitor clinic operations including, but not limited to:
-
Efficiency.
-
Coordination.
-
Supplies.
-
Equipment.
-
Physical plant issues.
-
Scheduling and access to care on a daily basis.
-
Identifying and addressing or elevating concerns regarding barriers.
-
-
The designated Supervising Registered Nurse (SRN) and the CME, or designee, shall meet weekly to review the PCTs’ performance, including, but not limited to, the overall quality and efficiency of services, health care outcomes, and level of care utilization. The review shall utilize tools such as Dashboards, Master Registries, Patient Summaries, and decision support tools to address or elevate issues as necessary.
-
-
-
Procedure
-
Determining Patient Risk
-
Automated Risk Classification System
-
CCHCS shall maintain an automated system that continuously updates a patient’s risk status based on the most current clinical information, including demographic, diagnostic, medication, specialty services, and inpatient data.
-
Within two calendar days of arrival at a Reception Center, all incarcerated persons shall be placed into the appropriate risk categories and be made available on the Master Registry. The Master Registry risk information shall be updated daily and made available to PCTs and other health care staff with need-to-know information (refer to Appendix 1, Clinical Risk Stratification Criteria).
-
-
Risk Verification
-
Each PCT shall be responsible for verifying that a patient has been placed at the appropriate risk level.
-
Any time a PCT member determines that a patient may have been placed in the wrong risk category, the team member shall elevate the issue using the established process. Refer to the Clinical Risk Verification Process available on the Lifeline Health Care Department Operations Manual Resources tab, for more detail on the communication process used to elevate discrepancies in risk classification.
-
-
-
Population Management Services Overview
-
Service Types and General Eligibility: CCHCS offers four levels of population management services (refer to Appendix 2, Population Risk and Resource Stratification Matrix):
-
Primary Prevention: Services to promote health, prevent onset of disease, and maintain current health status such as immunization and screening.
-
Secondary Prevention: Services to treat one or more well controlled diseases to avoid serious complications.
-
Tertiary Prevention: Services to treat the advanced stages of one or more diseases and minimize disability and includes complex care management services.
-
Catastrophic/Complex Care: Services may range from restoring health to only providing comfort care and includes complex care management services.
-
-
Primary Prevention Services Overview
-
PCTs are responsible for providing patients within the assigned patient panel services to promote, maintain and improve health, prevent disease, and identify and manage the early onset of disease. This level of services may be provided by Licensed Vocational Nurses, Psychiatric Technicians, and Registered Nurses (RNs) functioning within their respective scopes of practice, in collaboration with other members of the PCT. To fulfill this role, team members shall:
-
Remain current on preventive services guidelines, eligibility criteria, and the priority prevention areas listed in the State Health Care Services Performance Improvement Plan.
-
Use eligibility criteria, available registries and reports to identify and monitor subpopulations within the patient panel.
-
Directly provide preventive services including administering immunizations as well as screening and identifying and addressing risk factors by early interventions such as medications, lifestyle modifications, self-management tools, patient education, and other strategies to promote and maintain health.
-
-
Applicable Guidelines
-
PCTs shall provide Primary Prevention Services to the patient population based on age-gender recommendations from the United States Preventive Services Task Force Guide to Clinical Preventive Services and consistent with Care Guides.
-
PCTs shall utilize approved Nursing Protocols, Order Sets, Standing Orders, Care Guides, and other decision support tools when providing services.
-
-
-
Secondary Prevention Services Overview
-
PCTs are responsible for identifying and managing patients within the assigned panel who have one or more stable chronic diseases by providing services to halt progression and prevent serious complications. This level of services may be provided by RNs functioning within their scope of practice, in collaboration with other members of the PCT. To fulfill this role, team members shall:
-
Remain current on Care Guides issued by the Clinical Guidelines Committee, Nursing Protocols, Standing Orders, and other applicable evidence-based standards of care.
-
Be aware of identified priority chronic disease management areas listed in the Statewide Health Care Services Performance Improvement Plan.
-
Use available registries and reports to identify and monitor subpopulations within the patient panel eligible for disease management services.
-
Directly provide disease management services, including but not limited to, self-management planning and tools, patient education, routine ongoing evaluation of patient’s health status and progress toward self-management goals, and adjustment of treatment strategies and interventions.
-
-
Applicable Guidelines
-
PCTs shall utilize approved Nursing Protocols, Order Sets, Standing Orders, Care Guides, and other decision support tools when providing services.
-
PCTs shall reference other evidence-based guidelines if a Care Guide is not available for a specific condition.
-
-
-
Tertiary Prevention Services Overview
-
PCTs are responsible for identifying and managing patients within the assigned panel who are in advanced stages of one or more chronic diseases to stabilize current disease state, slow progression and to mitigate further complications as well as minimize disability and maximize functioning and independence. This level of services may be provided by RNs functioning within their scope of practice, in collaboration with other members of the PCT. To fulfill this role, team members shall:
-
Remain current on Care Guides issued by the Clinical Guidelines Committee, Nursing Protocols, Standing Orders, and other applicable evidence-based standards of care.
-
Use available registries and reports to identify and monitor subpopulations within the patient panel eligible for tertiary prevention services.
-
Directly provide tertiary prevention services, including but not limited to, routine ongoing evaluation of patient’s health status, adjustment of treatment strategies and interventions, reinforcing self-management planning and tools, patient education, and progress toward mutually agreed upon treatment goals.
-
-
Applicable Guidelines
-
PCTs shall utilize approved Nursing Protocols, Order Sets, Standing Orders, Care Guides, and other decision support tools when providing services.
-
PCTs shall reference other evidence-based guidelines if a Care Guide is not available for a specific condition.
-
-
-
Catastrophic/Complex Care Management Services for High Risk and Clinically Complex Patients Overview
-
High risk and clinically complex patients are at an exponentially higher risk for adverse health outcomes than the average incarcerated person and require more intensive assessment, monitoring, and treatment planning services to mitigate risk. Providing intensive services to this population is also an important utilization management (UM) strategy. While these patients comprise a small proportion of the total patient population (roughly ten percent), they consume more than half of the available pharmaceutical, specialty, and inpatient services. Although all PCT members shall have a role in complex care management, the Primary Care RN shall be the primary coordinator for complex care management services.
-
PCTs are responsible for identifying and managing patients within the assigned panel who have a very severe illness or condition and potentially significant risk factors. Services provided for these patients may have high costs with limited or no opportunity for improvement, stabilization, or cost control (e.g., end of life care, premature labor pregnancy complications). To fulfill this role, team members shall:
-
Remain current on Care Guides issued by the Clinical Guidelines Committee, Nursing Protocols, Standing Orders, and other applicable evidence-based standards of care.
-
Use available registries and reports to identify and monitor subpopulations within the patient panel eligible for catastrophic care services.
-
Directly provide catastrophic care services including, but not limited to, high intensity, direct, total and/or specialized care of complex, complicated, unstable or high risk patients.
-
Coordinate this level of services with the UM Nurse, CNE, CME, and Chief of Mental Health, or their respective designees, and ensure services are provided by a multi-disciplinary team of health care providers including specialists and specialized care settings.
-
-
Applicable Guidelines
-
PCTs shall utilize Care Guides and California Code of Regulations, Title 22, when providing services.
-
PCTs shall reference other evidence-based guidelines if a Care Guide is not available for a specific condition.
-
-
Eligibility for Services
-
Patients with the following risk designations shall be provided complex care management services:
-
High Risk 1.
-
High Risk 2.
-
Clinically Complex.
-
-
The PCT may elect to offer complex care management services to additional patients, including, but not limited to:
-
Medium risk patients with deteriorating health status.
-
Patients unwilling or unable to accept/participate in treatment.
-
Patients submitting multiple health care services requests for the same or similar complaints.
-
-
-
Multi-Disciplinary Plan of Care
-
All patients receiving health care services shall have a multi-disciplinary Plan of Care.
-
The Plan of Care shall be developed by the PCT; at a minimum, this includes the Primary Care RN and PCP. Other disciplines shall be included as indicated by the patient care needs.
-
Detailed discipline-specific plans shall be developed as indicated by patient needs and integrated with the overarching Plan of Care (e.g., Wound Care Plan, Pain Management, and Mental Health Treatment Plan).
-
The Plan of Care shall be documented and maintained in the health record.
-
-
-
Population Management Working Sessions
-
PCTs are responsible for providing the bulk of population management services for patients within their assigned panel.
-
The CME or Chief Physician and Surgeon and the CNE or SRN III, and others as appropriate to the institution’s mission and particular performance issues, shall hold working sessions conjointly with each institution Care Team at least twice monthly to ensure that teams have protected time to identify patient subpopulations and take action to address patient needs.
-
At a minimum, core PCT members shall attend the Population Management Working Session.
-
-
These working sessions offer a forum to:
-
Update PCTs regarding new clinical guidelines and organizational changes relevant to primary care delivery.
-
Identify barriers to care and resource needs.
-
Provide PCTs regular feedback about their performance in managing clinic work, coordinating patient services, and evaluating Care Team performance.
-
Assist Care Teams in managing subpopulations within the patient panel and improving patient outcomes.
-
-
Topics shall include, but are not limited to:
-
Patient registry flags and alerts indicating abnormal clinical findings and/or missing documentation (e.g., CDCR 1845, Disability Placement Program Verification, CDCR 7410, Comprehensive Accommodation Chrono, Medical Classification Chrono, Medical Hold).
-
Trends in the PCT’s performance on key Health Care Services Dashboard metrics as compared to statewide performance objectives, the statewide average, and the performances of other Care Teams at the institution.
-
Utilization of resources including, but not limited to, supplies, equipment needs, and contracts.
-
Access to care data and statistics.
-
Scheduling Reports (e.g., Aging Report, To Be Scheduled Report).
-
Potentially avoidable hospitalizations for any patients within the panel.
-
New patients and patients leaving the panel in the context of their impact on the overall risk stratification of the patient panel (workload management and resource demand).
-
Mission changes that impact the patient panel (e.g., yard conversions, constructions, new programs).
-
-
-
Sustainability of Population Management Services
-
Key Roles in Population Management and Patient Panel Allocation
-
Institution leadership shall periodically review the roles and responsibilities of staff providing oversight or delivering population management services including, but not limited to:
-
PCT members.
-
Clinic operations supervisor.
-
Public Health Nurses.
-
UM Nurses.
-
Unit supervisors.
-
Penal Code 2602 coordinators.
-
Enhanced Outpatient Program coordinators.
-
-
Institution leadership shall ensure procedures, templates, and roles and responsibilities are updated as new tools and technology become available.
-
Institution leadership shall periodically review the composition of patient panels, particularly relative to the number and proportion of patients that fall into each risk category, to ensure available staff resources are distributed in order to provide the required population management services.
-
-
Training and Decision Support
-
The CEO and institution leadership team shall establish an orientation and training program to ensure all staff serving as members of a PCT or supporting Care Team functions fully understand their roles and responsibilities prior to assuming their duties including, but not limited to:
-
Review of the expectations in this procedure.
-
Changes to local population management processes.
-
National health care industry advances pertinent to the Patient-Centered Health Home.
-
New information systems or technology that may increase the efficiency or effectiveness of Care Team processes or forums.
-
Updates in clinical practice, including new CCHCS clinical guidelines, standing orders, nursing protocols, industry best practices, and findings in clinical literature.
-
-
During twice-monthly Population Management Working Sessions and in other forums, institutions shall provide staff involved in population management with training and information to support staff in providing high quality care, including, but not limited to:
-
New guidelines and procedures.
-
Use of new technology and tools.
-
Effective processes and strategies in preventive care, disease management, and complex care management.
-
Best practices in the health care industry relative to population management, especially in the area of handoffs/communication across different health care settings.
-
Common system lapses in the area of population management and ways to prevent these lapses from occurring.
-
Group review of specific patient cases for problem-solving and education.
-
-
Institutions shall assess the competence of staff performing population management work at least annually. Results shall be documented in the employee file and staff development training file.
-
-
Performance Evaluation and Improvement
-
Designated Standing Improvement Committee
-
Institution leadership shall designate an existing interdisciplinary standing committee reporting to the local Quality Management Committee (QMC) for oversight of the population management system monitoring activities.
-
-
Evaluation
-
The committee shall review population management performance trends and take action to improve care at least monthly. At a minimum, the committee shall review Health Care Services Dashboard information but may also consider monitoring reports, internal audits and surveys, and reviews by stakeholders such as court experts, the Prison Law Office, and the Office of the Inspector General. Beyond trends in performance metrics, the committee shall also consider the quality and effectiveness of program infrastructure, including, but not limited to:
-
Culture of excellence and teamwork.
-
Communication between PCT members, PCTs, health care staff and custody, and with providers in other health care settings.
-
Health information flow, including registry and Patient Summary usage.
-
Resource allocation in accordance with panel composition.
-
The extent to which daily huddle, Population Management Working Sessions, and Care Plan Conferences satisfy the purpose and requirements outlined in this procedure.
-
Competency of staff in key population management roles.
-
Decision support.
-
System for orienting and developing staff.
-
Program monitoring and staff competency testing.
-
-
Committee Actions
-
The committee may take a number of actions to improve program performance, including, but not limited to:
-
Identifying and prioritizing areas for improvement in population management.
-
Setting performance objectives.
-
Establishing improvement teams and/or directly managing improvement initiatives.
-
Applying nationally-recognized improvement techniques to analyze quality problems and develop and test solutions.
-
Monitoring the progress of improvement initiatives at least monthly and intervening as necessary when initiatives stall or show a decline in performance.
-
Identifying best practices and disseminating them across the institution.
-
Documenting improvement activity and results.
-
Regularly reporting performance trends and improvement activities to the QMC.
-
Ensuring that staff working in population management has the knowledge and skills necessary to contribute to improvement activities.
-
-
-
-
Appendices
-
Appendix 1, Clinical Risk Stratification Criteria
-
Appendix 2, Population Risk And Resource Stratification Matrix
-
-
References
-
California Code of Regulations, Title 22, Division 5, Chapter 12, Correctional Treatment Centers
-
California Penal Code, Part 3, Title 1, Chapter 3, Article 1, Section 2602
-
United States Preventive Services Task Force Guide to Clinical Preventive Services
http://www.ahrq.gov/professionals/clinicians-providers/guidelines-recommendations/guide/index.html -
Agency for Healthcare Research and Quality – Patient Centered Medical Home Resource Center, Patient-Centered Medical Home | ACT Center (act-center.org)
-
The Joint Commission Primary Care Medical Home Certification, http://www.jointcommission.org/accreditation/pchi.aspx
-
National Committee for Quality Assurance – Patient-Centered Medical Home Recognition, http://www.ncqa.org/Programs/Recognition/Practices/PatientCenteredMedicalHomePCMH.aspx
-
Commonwealth Fund – Safety Net Medical Home Initiative, http://www.commonwealthfund.org/interactives-and-data/multimedia/videos/2011/safety-net-medical-home-initiative
-
Robert Wood Johnson Foundation & John Hopkins Bloomberg School of Public Health/Chronic Care: Making the Case for Ongoing Care: Chronic Care: Making the Case for Ongoing Care (jhu.edu)
-
Accelerating Care Transformation (ACT) Center, Kaiser Permanente Washington Health Research Institute: Reducing Care Fragmentation: A Toolkit for Coordinating Care: https://www.act-center.org/application/files/7016/3112/2157/Toolkit_Reducing_Care_Fragmentation.pdf
-
-
Revision History
-
Effective: 06/2016
-
-
Appendix 1: Clinical Risk Stratification Criteria
Risk Category Definition Complex Care High Risk 1 Patients who trigger at least 2 of the following high risk selection criteria:
∙ High Risk Diagnosis/Condition: associated with current or future risk for adverse health event
∙ Multiple Higher Level of Care Events:
– Medical – 2 or more community hospital admissions in the past 12 months
– MH – 3 or more MH higher level of care admissions in the past 12 months
∙ Prolonged Medical Bed Stay: patients in CRC, OHU or a SNF≥50% of the past 90 days
∙ Polypharmacy: patients on 10 or more medications
∙ High risk specialty consultations (e.g., oncologist, vascular surgeon)- 2 or more in past 6 months
∙ 65 years of age or older
∙ Co-Morbid Medium Risk Diagnoses/Conditions: a combination of “medium risk” conditions which can be additive to increase the risk for future adverse health care events. (e.g., CKD with DM)Patients who meet one or more of the following criteria:
∙ Any mental health level of care higher than CCCMS
∙ Risk level of High Risk 1 or 2
∙ 2 or more admissions to a mental health higher level of care in the past 6 months
∙ Polypharmacy (taking 10 or more medications)
∙ Any hospitalizations in the past 3 months
∙ On medical hold
∙ Special Outpatient Program statusHigh Risk 2 Patients who trigger at least one of the high risk selection criteria listed under “High Risk 1” above. Medium Risk Patients with at least 1 chronic condition who do not meet the selection criteria for high risk; includes patients enrolled in the Mental Health Services Delivery System and patients with permanent disabilities (under ADA) affecting placement. Low Risk Healthy patients who do not meet any of the selection criteria for medium or high risk; includes a subset of patients with well-managed/stable chronic illness. -
Appendix 2: Population Risk and Resource Stratification Matrix
Category LEVEL 1:
Primary Prevention
(Low Resource Use)LEVEL 2:
Secondary Prevention
(Moderate Resource Use)LEVEL 3:
Tertiary
(High Resource Use)LEVEL 4: Catastrophic/Complex
(Very High Resource Use)Clinical Risk Low Risk Medium Risk High Risk 2 High Risk 1 Goal To prevent onset of disease and maintain current health status. To treat a disease and avoid serious complications. To treat the late or final stages of a disease and minimize disability. May range from restoring health to only providing comfort care. Healthy patients with no known diagnosis or complex treatments; however, may demonstrate warning signs or potentially significant risk factors.
Example:
∙ Healthy
∙ Blood glucose and lipids rising, but still within desired parameters.
∙ BMI elevated
∙ Smoker
Includes some patients with medical or mental health conditions considered to be well controlled or at low risk for adverse health event.
Example:
Otherwise healthy patients, including:
∙ Those who use ≤ 2 SABA dispenses in 12 months and not on an ICS
∙ Those with all HgA1C < 7.7 in 12 months and not on insulin
∙ Those who only receive monotherapy for blood pressure management
∙ Those who are receiving treatment for LTBI and have AST < 2Xs normal elevation
∙ CCCMS without medications or on a KOP SSRI only
Basic, uncomplicated nursing care of largely well population; prevention and wellness; stable, uncomplicated chronic disease; episodic care of acute injury or illness; routine care in primary care clinic; annual or semi-annual patient service plans (PSP).
Example:
∙ Independent ADLs
∙ Short term (no more than 4 weeks duration) conditions
∙ KOP medications or medication line no more frequent than BID
∙ Vital signs monthly, vital signs weekly for short period of time (no more than 4 weeks duration)
∙ Labs/procedures/treatments performed no greater than monthly except for situations as specified for short-term (no more than 4 weeks duration) medical conditions
∙ Independent wheelchair user and engaged in self management without complications.
Note: incarcerated person should be in an ADA designated facility.
∙ Independent prosthetic devices and engaged in self management without complications.
Note: incarcerated person should be in an ADA designated facility.
∙ Attend activities independently and willingly
∙ No thought disorder; no withdrawn or intrusive behavior
∙ Oriented, interacts appropriately
∙ Manages incontinence including indwelling catheters
[Most low risk patients will fall into this level/category.]Have diagnosis and/or complex treatment; at higher risk for complications or potentially significant risk factors.
Example:
∙ Blood sugar and lipids not within desired parameters
∙ No support system
Includes patients with at least one chronic condition or mental health condition at higher risk for adverse health event.
Example:
∙ One or more chronic illness, based upon prescribed medications and/or laboratory tests.
∙ CPAP with oxygen at night only
∙ Episodic oxygen therapy for acute asthma or respiratory condition no greater than twice a month
∙ CCCMS on NA/DOT medications
∙ MH High Utilization
∙ Permanent ADA with history of/or current complications
∙ Pregnancy
Low intensity nursing care of stable, chronic disease; functional limitations compensated by adaptive equipment; maintenance of status; prevention of exacerbation; symptom control and pain management; uncomplicated wound care (time-limited); uncomplicated chemo/radiation therapy; Quarterly patient service plans (PSP).
Example:
∙ Independent in ADLs
∙ Stable, chronic disease
∙ Routine Medication Line: NA/DOT, injectable and or transdermal medications. May also have KOP medications.
∙ PRN Medications: requires oral PRN medications including narcotics for significant physical symptoms.
∙ Vital signs daily for short period of time (not to exceed 2 weeks) to ascertain stability excluding vital signs required for certain medication such as pulse before administering Digoxin.
∙ Vital signs no greater than weekly excluding vital signs taken as required for certain medication such as pulse before administering Digoxin.
∙ Labs/procedures/treatments performed no greater than weekly for stable chronic disease excluding diabetic checks.
∙ Prosthetic devices with minimal assistance.
∙ Thought disturbance, effectual disturbance, withdrawn or intrusive behaviors requiring only redirection.
∙ Independent management of colostomies, incontinence including catheterization, and tracheotomies
∙ Wound care: uncomplicated, time-limited wound care or chronic stasis ulcers with independent dressing changes.
[Most medium risk patients will fall into this level/category.]Has diagnosis, complex treatment, and complications or potentially significant risk factors-goal is to prevent further complications.
Example:
∙ Has diabetes with early renal disease, coronary artery disease, failing eyesight and no support system.
∙ Three ER visits and two hospitalizations in past year
∙ Needs assistance with ADLs
Includes patients who are high risk priority 2 and trigger only 1 flag from the selection criteria below:
Example:
∙ Medications associated with important diagnoses which, if not taken, may lead to a serious adverse event (e.g., immunosuppressant, chemotherapy)
∙ 2 or more inpatient admissions in a 12 month period
∙ 2 or more appointments to “high risk” specialist(s) (e.g., oncologist, vascular surgeon) in a 6 month period
∙ 65 years of age or older
∙ 3 or more Mental Health Higher Level of Care admissions in the last 12 months
∙ In the CTC, OHU or SNF for 50% or more of the last 90 days
∙ Prescribed 10 or more medications
Medium intensity nursing care of complex, stable or at risk patients; uncomplicated post-surgical care; dementia, paraplegia, or hemiplegia able to participate in self-care; uncomplicated wound care (high risk for skin breakdown); Outpatient Housing Unit (OHU) placement; Monthly or every 2 month patient service plans (PSP).
Example:
∙ Requires some assistance with ADLs (bathing, feeding, dressing, toileting, etc.)
∙ Unstable, chronic disease, may require OHU placement
∙ Routine Medication Line: 3 or more NA/DOT, injectable and or transdermal medications. May also have KOP medications.
∙ PRN Medications: requires oral PRN medications including narcotics for significant physical symptoms.
∙ Colostomy and/or Foley catheter care requiring nurse intervention. If patient is stable and treatment is ongoing consider for placement in LTC facility.
∙ Frequent incontinency requiring nursing intervention – criteria for LTC
∙ Episodic incontinence including colostomies and indwelling catheters requiring nursing intervention – criteria for unstable chronic disease.
∙ Initiation of involuntary medications
[Most high risk priority 2 patients will fall into this level/category.]Have very severe illness or condition and potentially significant risk factors. May have high costs with limited or no opportunity for improvement, stabilization, or cost control (i.e., end of life care, premature labor pregnancy complications).
Example:
∙ Diagnosed with lung cancer
∙ Recent myocardial infarction
∙ Progression to ESRD with renal dialysis
∙ Amputation of one leg
∙ Blind
Includes patients who are high risk priority 1 and trigger at least 2 flags from the selection criteria below:
Example:
∙ Medications associated with important diagnoses which, if not taken, may lead to a serious adverse event (e.g., immunosuppressant, chemotherapy)
∙ 2 or more inpatient admissions in a 12 month period
∙ 2 or more appointments to “high risk” specialist(s) (e.g., oncologist, vascular surgeon) in a 6 month period
∙ 65 years of age or older
∙ 3 or more Mental Health Higher Level of Care admissions in the last 12 months
∙ In the CTC, OHU or SNF for 50% or more of the last 90 days
∙ Prescribed 10 or more medications
High intensity, direct, total and/or specialized nursing care of complex, complicated, unstable or high risk patients; daily care plan updates; significant dementia, paraplegia, hemiplegia, or quadriplegia unable to participate in self-care; Care management required; Inpatient level of care.
Example:
∙ Requires significant assistance or total care with ADLs (bathing, dressing, feeding, toileting, turning and positioning, ambulation and range of motion)
∙ Level of Care: Acute medical or mental health inpatient, skilled nursing facility, LTC facility, Hospice or end of life care.
∙ NA/DOT medications only
∙ IV therapy, blood and blood product transfusion, IV meds
∙ Daily vital signs, procedures or treatments for acute and unstable chronic disease excluding diabetic checks.
∙ Severe ill effects from chemotherapy and/or radiation therapy
∙ Complicated wound care to include use of wound vac.
∙ Frequent suctioning
∙ Tracheostomy with extensive nursing intervention
∙ NG tube or G-tube feedings requiring total nursing intervention
∙ Routine incontinence requiring total nursing intervention.
∙ Colostomy and/or Foley care that must be done by nurse
∙ Medical restraint (posey, soft wrist restraints, etc.) required for protection of self or to stabilize medical devices/dressings/tubes
∙ Confusion and disorientation secondary to dementia
∙ Thought disturbance, effectual disturbance, withdrawn or intrusive behavior that requires seclusion or restraint for protection of self and others
∙ Self-injurious behavior, 1:1 observation (acute mental health only)
∙ High Risk Pregnancy
[Most high risk priority 1 patients will fall into this level/category.]